THE POST WAR PERIOD
Again, Vera Wilson's account of this time can hardly be bettered:
In 1945 the Bristol Health Committee took over the control of Frenchay General Hospital as agents for the Ministry of Health, on the understanding that the hospital was made suitable for civilian purposes. The Ministry of Works carried out some reconstruction, but there was still much to be done when the first hospital team arrived on the premises.
A few of the buildings were derelict, and the huts where the American troops had lived were packed with stores and equipment, most of which was unsuitable for use in a civilian hospital.
The gardens and grass verges were unkempt, and rubble had been dumped in large mounds, mainly in the Lime Tree Avenue.
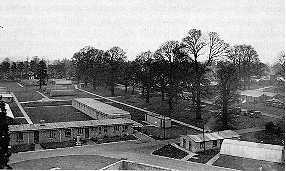
The wards of the former E.M.S. hospital were built onto two sloping, open-sided corridors or ramps, 330 yards long, each ward separated from its neighbour by a paved garden or grass lawn. The buildings were of brick construction, some with flat hollow concrete roofs and the remainder with steel-trussed gable roofs. The floors were of bitumastic material laid on a concrete base which had proved to be unsatisfactory. The lighting and heating were inadequate and the whole appearance of the hospital was bleak.
During the Second World War a Thoracic Surgery Unit had been set up at Kewstoke Emergency Hospital. This Unit was transferred to Frenchay in April, 1946, and was the first clinical department to occupy the Frenchay site after it was vacated by the United States forces. The Thoracic Team took possession of six wards, the two operating theatres, and some ancillary premises. The Consultant Thoracic Surgeon appointed in charge of the Unit was Mr R.H.R. Belsey, M.S.,F.R.C.S.
In 1948 George Alexander, F.R.C.S was appointed as
Consultant Neurosurgeon and he began to set up the Regional
Neurosurgery Unit. Later in 1948 the N.H.S. came into being. This was a
major change in the way health care was to be delivered. There was much
talk of the 'appointed day', i.e. the day the Service came into
existence. However, the N.H.S. didn't come unannounced, a lot of
background work had been undertaken in the years leading up to 1948.
[In 2009 Katy Gilkes MRCS,
neurosurgical registrar at Frenchay, alerted me to the founding role
played by Diane Beck. DB was arguably the world's first female
neurosurgeon. In 1943 she was appointed as a consultant to the
Emergency Medical Service in southwest England; she was based at the
Burden Institute, then associated with the Stoke Park hospital complex
. The Emergency Medical Service took it over during the war as a venue
for managing neurosurgical casualties from the region. After the war,
the neurosurgical service was transferred to Frenchay Hospital, forming
the basis of today's unit.]
In 1951 John Sage, the Deputy Secretary of the 'new' Frenchay Hospital,
as it had come to be known, previously having been 'Frenchay Park
Hospital', wrote a pair of articles in 'The Hospital', the then Journal
of Hospital Administrators. When I approached him personally in 1990 or
so to ask if he had copies of his own articles he had none; however the
successor Journal to 'The Hospital' had copies in London and they
kindly supplied me with photocopies. His contemporary account must be
the most authoritative of the period:
The three years which have passed since the appointed day have witnessed at Frenchay Hospital a degree of expansion of existing services and development of new departments which, for a hospital of its kind, can hardly have been surpassed.
On 5th July 1948, the Frenchay Park Estate consisted of Frenchay Park Children's Orthopaedic Sanatorium, Frenchay General Hospital and Frenchay Farm together with some ninety-five acres of arable land, pasture and amenity gardens. The Sanatorium was founded in 1921 when the Bristol Corporation purchased a charming Georgian building, formerly the Mansion House, with its surrounding parklands. Extensions in 1931 provided 98 beds in three very pleasant detached wards of the veranda type. Frenchay General Hospital, planned in 1938 under the Emergency Medical service, was built early in the last war on the pavilion system, and occupied by the U.S. Army. In 1945, the hospital was placed under the control of the Bristol Health Committee as agents for the Ministry of Health. When the management committee assumed control the bed complement was 530, of which 206 were staffed and in use by regional units of thoracic surgery (90 beds), neurological surgery (40 beds) and venereal diseases (42 beds) plus two wards for female chronic sick and male non-surgical tuberculosis of 18 and 16 beds, respectively. A further 78 beds were devoted to a residential nursery unit of the Bristol Corporation, while other accommodation housed an intensive training school for male nurses under the aegis of the Ministry of Health and a temporary health centre. Vast stocks of American equipment, most of which was sub-standard to civilian hospital requirements, occupied various buildings on the estate.
[After the War wards 14, 15 and 32 were used as a Corporation of Bristol children's residential nursery. (Later ward 32 was renumbered as 27; "32" was still plainly visible next to the door frame in 1995!). Frenchay House and Frenchay Lodge, both on the Common, were also part of this complex. Nursery nurses were trained at Downend Children's Home and sent to the nursery as part of this training. Some of the children were orphans; others had American fathers. They were all healthy and were not part of the TB hospital.]The first steps taken by the committee at their initial meeting was to declare the two institutions administratively one entity, and the process of fusion was gradually completed during the following months by amalgamation of departments at all levels with sectional heads appointed to the combined hospital. It is not the object of this paper to discuss administration or staff organisation, but it may be mentioned in passing that the following principal officers are now responsible in their respective spheres for the whole hospital - Matron, chef-de-cuisine, group engineer, domestic supervisor, superintendent radiographer, superintendent physiotherapist, head occupational therapist and head store keeper.
Development Policy
From the start it was the policy of the newly-constituted management committee to develop at Frenchay an institution worthy of a place in the front rank of general hospitals and nurse training schools. It was evident that to transform an E.M.S. hospital, planned and fitted on a wartime standard, with half its wards empty and in a state of internal dilapidation, into an up-to-date general hospital adequately furnished and fully occupied, with the necessary residential staff quarters - all this would require considerable effort and the expenditure of large sums of money. It was equally evident that having regard to prevailing economic conditions and shortages of raw materials, higher authority would need to be not only convinced that Frenchay Hospital ought to be developed, but must also be imbued with some sense of urgency - one might say even enthusiasm.
The planning of this project could be seen to fall broadly under the following headings:
(a) Improvement of the standard of the whole of the existing ward accommodation and certain ancillary departments, and development of the hospital to its full capacity (the introduction of general medicine and general surgery being essential).
(b) Establishment of a complete nurse training school.
(c) Provision of the residential staff quarters which these developments would demand.
The programme the committee set itself was indeed a formidable one and might well have been expected to unfold but slowly over a period of many years. It is a remarkable achievement that the keen and sustained effort of the management and their chief advisors has brought the project, within three years, at least halfway towards the ultimate goal.
It will be appreciated that the objectives enumerated above were not individual problems to be tackled in isolation or separate stages of development which might be worked on and disposed of seriatim. Each had bearings on the others and each had to dovetail at all times so that the master-plan might develop in a coherent and balanced manner. Moreover, from the purely practical point of view of nursing staffs and ancillary departments, a considerable amount of movement of wards and re-allocation of residential accommodation has been unavoidable and this inconvenience will continue for many months to come. Close liaison has always existed, however, between the administration and the senior staff of all sections and information on the progress achieved and imminent developments is disseminated as appropriate from time to time.
When reviewing one by one the component parts of this undertaking it must be borne in mind that they were all on the move simultaneously. Discussions among officers, meetings of committees, conferences at regional board and Ministry level, round the table and on site, have been taking place almost daily. An attempt will be made in the following paragraphs to outline the more interesting features of the enterprise.
Modernisation and Development
Experience at Frenchay leads one to the conclusion that building a new hospital - in other words, putting complete plans on paper of exactly what is wanted and then erecting from ground level the wards, theatres, ancillary departments and nurses' homes, all of which have been designed as complementary one to another - is far easier than modernising and refitting a partially occupied and ill-balanced institution.
What progress has been made? At the appointed day the bed complement of the amalgamated institutions (which it was decided should be known simply as Frenchay Hospital) was 630 of which 304 only were staffed as hospital beds. Having reviewed the available accommodation for patients, the committee laid down the following allocation of beds, which is designed to present ultimately a well-balanced institution for the treatment of the sick and teaching of student nurses.
No. of Number of beds
wards Surgical Medical
Neurological surgery 4(2) 80(36)
Thoracic surgery 6(6) 120(108)
Plastic Surgery 5(4) 120(85)
General Surgery 5(2) 100(40)
General Medicine 8(5) -- 160(110)
(including TB)
Venereal Disease 2(2) -- 40(40)
Isolation and Staff 1(1) -- 10(10)
31(22) 420(269) 210(169)
Figures in bracket indicate beds in use at 1st July 1951.
The reader will gain a clearer picture of the magnitude of the task if each section of the hospital is described, very briefly, as the new management committee found it, following which a few notes will be given on the progress to date.
All the buildings of the former emergency hospital are single storey, fifteen of the wards being of brick construction with flat roofs of hollow concrete, the remaining thirteen of brick with gabled roofs of steel truss type. The wards are built on to two covered (but open-sided) sloping corridors or ramps, each 330 yards long, each ward being separated from its neighbour by grass lawns. Covered ways (also open-sided) connect the two ramps. The ward picture in July, 1948, was indeed a depressing one. Heating was provided by anthracite stoves - one need not elaborate on the undesirability of making up solid-fuel fires and raking out ashes in surgical wards. The ward floors were of a bitumastic material with concrete base. Laid down at a time when this preparation was at an experimental stage it proved unsatisfactory, becoming indented (with disconcerting rapidity) from the weight of the bedsteads and other furniture. Dust pockets form in the resultant potholes which defy cleaners and cause surgeons no little anxiety. The ward lighting left much to be desired, the points provided being not only insufficient in number, but also inconveniently positioned. No private or even semi-private rooms were available, the open ward unit of 18 or 20 beds being the only accommodation available even for patients who might, on medical grounds, be in need of quiet and seclusion.
As long ago as 1946 when discussions first took place between the Ministry of Health, Ministry of Works, the University of Bristol and the Local Authority on future development at Frenchay, preliminary plans had been formulated for a complete central heating scheme. Progress was disappointingly slow and various factors caused modifications of the original proposals from time to time. Complete agreement was not reached until late in 1949 when the whole position was reviewed in the light of authority recently received to the preparation of plans for a new nurses home (referred to later). Final Treasury approval was received by the Ministry of Works in September,1950, and the first stage of the scheme commenced in October. The building of an additional boiler house is required and is scheduled for completion by October, 1952. Happily the existing main boiler house has sufficient capacity to provide a hot-water circulation to thirteen wards and the first of these fortunate units enjoyed central heating during the second half of last winter. The installation of radiators is progressing apace and it is confidently hoped that the last will be seen of solid fuel stoves by October, 1952!
Proceeding side by side with central heating is the relaying of all ward floors and general modernisation of the thirteen wards of gabled type. Phase I of this work - involving six wards only -was agreed with the Ministry of Works long before the appointed day, but had been held up pending Treasury approval. This was forthcoming in August, 1950, since when these wards have been completed and occupation taken, the last being put into commission on 2nd April, 1951. Meantime, in September, 1950, financial approval was received to the modernisation of the remaining seven of this type of ward. This modernisation makes provision for new suspended ceilings and complete rewiring of the electrical installation to give a separate light over the bed of each patient - a desideratum previously lacking throughout the hospital - together with the fitting of French casements to enable bed patients to be wheeled on to the surrounding terraces. As regards private rooms, these have so far only been built in the four wards allocated to neurosurgery, where the medical need may be said to be most urgently necessary. These rooms, three per ward, are of brick and are sound insulated. It is hoped to incorporate similar private rooms in all wards as the main scheme proceeds, and at the same time to provide curtained cubicles in the public portion of each ward to give adequate privacy when required, and to obviate the need for portable screens.
Neurosurgery and Plastic Surgery
The provision of a new permanent neurosurgery theatre had been agreed in principle in 1946. Not until late in 1948 was it possible to proceed with detailed planning. After representations by the Director of the Neurosurgical Unit, Ministry of Health approval was obtained to a twin theatre layout incorporating glass screened balconies for spectators. The need for two theatres is considered essential in this type of case as major operations in neurosurgery may last many hours. Should an emergency head injury present itself a delicate situation is liable to arise. Final Treasury blessing for this project having been received in August last, the work is scheduled to commence in the fall of this year. As a preliminary phase in building up a comprehensive Neurosurgical unit the existing X-ray department has recently been expanded by the addition of a Schönlander skull apparatus and a new suite containing examination and perimetry rooms and secretarial offices was made available for use in January, 1951. The whole scheme will provide at Frenchay what is considered to be the most up-to-date Neurosurgical unit in the country.
For some years prior to the appointed day the University of Bristol had been endeavouring to establish a Department of Jaw and Plastic Surgery to complete the arrangements for specialised units in the Bristol area.
As early as July, 1948, the management committee, at the request of the regional board, appointed an ad hoc committee to examine the proposal to accommodate such a unit at Frenchay Hospital. With very little delay a scheme was formulated to establish a jaw and plastic surgery department in the wards and theatre hitherto occupying the children's orthopaedic sanatorium, the accommodation to consist of three wards of 20 beds, and two wards of 30 beds (including a burns unit) with double operating theatres. However, it was found that planning and finance delays would not permit the project to keep pace with the increasing waiting list of cases and the management decided that a measure of improvisation was demanded. By adaptation and refitment of the existing single theatre the unit was opened in October, 1949, with 70 beds. It was hoped that the permanent scheme would be commenced on 1st April, 1950 - however, a further blow to the committee's hopes was given by a retrenchment of capital expenditure and new building has had to be postponed. Disturbed by the ever growing waiting list - then standing at 500-600 - the committee decided in May, 1950, on further adaptations within the existing theatre accommodation designed to permit increased operating sessions and the opening of a further 15 beds. These minor conversion works have been very skilfully designed to form par t of the architect's plans for the permanent twin theatres, and are now making possible the very urgently required increase in turnover of plastic surgery cases. [Geoffrey FitzGibbon, F.R.C.S was appointed Consultant Plastic Surgeon in 1949].
An essential adjunct to a jaw and plastic surgery unit is a dental department. The establishment of a dental department at Frenchay as part of the arrangements for plastic surgery was approved by the regional board in May, 1949, and planning of this unit proceed side by side with the main scheme. It was decided to adapt and renovate the building formerly used for the same purpose by the American Army. The work commenced the first week in February, 1950, and was completed by the end of June. Three surgeries are provided, with laboratory, plaster room, darkroom and adequate waiting accommodation. [W. Bakewell L.D.S. was appointed Consultant Dental Surgeon at this time].
Photographic Unit
In June, 1949, the Clinical Photographic Service Joint Committee of the University of Bristol, the South Western Regional Hospital Board and the United Bristol Hospitals gave consideration to the question of extending the service by setting up at Frenchay Hospital a sub-department of the main unit situated at the Bristol Royal Hospital. This department would deal locally with the work required by the thoracic and neurosurgery units and the large additional amount of work which would be provided by the establishment of plastic surgery at the hospital. The management committee readily agreed with the proposal and the building in use as the hospital sewing room was designated for the purpose. Though this involved yet another re-allocation of accommodation (an event borne at frequent intervals by many sections of the hospital during this prolonged period of 'growing pains' - and accepted with a resigned cheerfulness by the staff concerned!) it was thought advisable that the photographic unit be sited adjacent to the plastic surgery wards and the dental department, while still being accessible to other sections. The unit opened in mid-1950, the photographer-in-charge being deputy to the head photographer at the Bristol Royal Hospital.
General Surgery
Prior to the appointed day, planning for the new Frenchay Hospital had proceeded on the assumption that an exclusively specialised hospital would be developed. It later became apparent that such a conception is unpractical. A hospital conceived on such a basis cannot find the necessary nursing staff and even in affiliation cannot adequately fill its proper place as a training ground for student nurses. The provision of general medicine and general surgery wards was therefore a sine qua non. Moreover, the surgical waiting list in the Bristol area is of the order of 2,000-3,000.
With these considerations in mind the management committee, within six months of their taking office, formulated plans for broadening the scope of the hospital by allocating 100 beds for general surgery and earmarking a site for theatre accommodation. This unit is to be provided by adaptation of a building formerly used as a games room and will consist of twin operating theatres with anaesthetic rooms, sterilisation and all other ancillaries.
Plans were approved and finance made available by the regional board in November, 1949, and a tender for the work was accepted by the management in January, 1950. The economic veto of expenditure on capital schemes, with which all hospital administrators are so familiar, then descended like a wet blanket and stifled any further progress until late November, when after several false alarms the final word was given and work commenced on twenty-third of that month. The department opens 1st August, 1951.
Meantime, in November, the regional board had appointed a general surgeon [R. Gordon Paul F.R.C.S.E.] whose duties will be principally in the Cossham-Frenchay Group and the management, quick to seize the opportunity thus presented, arranged for the immediate allocation early in January, 1951, of one ward of 20 beds and by temporary improvisation of the theatre facilities the introduction of general surgery at Frenchay has been made possible and more beds are available for teaching purposes. A second ward was opened in April. With the imminent completion of the new theatres further beds will be placed at the disposal of the general surgeons later this year.
Out Patients and Casualty
A short note is necessary regarding the reconstruction of a Health Centre on the hospital estate in conjunction with a casualty and out-patient department. The area around the hospital, though as yet, on the Gloucestershire side, largely rural, is becoming built-up rapidly on the south and east by the expanding housing estates of the Bristol Corporation. Long before the appointed day the local authority conducted ante-natal and infant welfare clinics in improvised accommodation in a hospital ward. It was clear in 1948 that hospital development would, in course of time, render this arrangement impracticable. At the same time the hospital medical staff were pressing for improved out-patient clinic facilities and it was obvious to the management that the expansion of the existing specialities and introduction of general medicine and surgery would demand a properly sited and adequately furnished casualty department. Ideal premises were found in a former officers' mess adjacent to the main gate and consisting of two buildings with a connecting corridor.
The first of these has been reconstructed by the local health authority who took occupation in July, 1950. Adaptations to the remainder were completed in January, 1951 - meantime the hospital consultant staff conducted out-patient sessions in the health centre. A happy arrangement has been concluded between the Corporation and the management for joint administration and the widest possible mutual use of the whole of the premises. The casualty side of the work is expected to expand slowly during the next six months though full facilities cannot be given to the surrounding population until the hospital's general surgery department is opened.
Staff Sick Bay
Lastly, the provision of a staff sick bay is worthy of record. This was made available in June, 1950. Before that date sick staff could only be accommodated, if sufficiently ill, in one of the hospital wards otherwise they were treated in their own rooms, neither method being satisfactory. A small ward of the former sanatorium, providing ten single rooms, seemed ideal and after minor alterations, was brought into use for the purpose. Here the senior resident medical officer carries out pre-employment examinations, Mantoux tests, etc., and has her staff patients under her eye at the same time.
Kitchen Accommodation
Having dealt, albeit somewhat sketchily, with the wards, theatres and other clinical departments, one may turn to a brief review of certain ancillary services. Of no less importance than good medical attention and nursing, though possibly sometimes overlooked, is good feeding which in turn is dependent primarily on good cooking, but also on adequate equipment. The state of the main kitchens of the hospital in July, 1948, left much to be desired. The equipment no doubt was satisfactory as a wartime expedient in a temporary military hospital, but could not be looked upon as in any way approaching the standard expected under peacetime civilian conditions. The main oven was of the double-banked coal-fed type - very out-of-date, inefficient and dirty in working and firing; an electric griller and fish-fryer and steam ovens were also considered inadequate for the numbers to be catered for even at that time and would be quite unable to cope with the fully developed hospital. A comprehensive report by the newly-appointed chef-de-cuisine recommended an extensive programme of re-equipping and reorganisation of the general layout of the kitchens.
The catering sub-committee was charged in February, 1949 with the duty of examining the existing facilities and submitting proposals designed to build up a satisfactory service for feeding both patients and staff, bearing in mind the long-term programme of development to 630 beds which the management had laid down. It was decided to obtain expert advice and several firms of catering engineers were invited to prepare schemes for modernisation of the hospital kitchens. Much detailed discussion was involved in a scheme of this kind, including a long series of meetings on site, and though a final recommendation to the board was not made until December,1949, actually there had been no avoidable delay. The committee's proposals provided for the installation of new roasting and steaming ovens, boiling pans, gas-fired range and fish-fryer; mixing machines and many minor accessories all, where appropriate, of stainless steel; new extract ventilation plant with Georgian wire glazed canopies and new mains for steam, condense, water and gas - the total cost being £6,900. The board's approval was obtained in January,1950, work commenced in February, and was completed in slightly less than twelve months. The finishing touch was given to what in essence is a new kitchen when the whole building was redecorated in February, 1951. This kitchen will feed an ultimate total of some 900 patients and staff.
Gas Supply
The reader will have noted that reference has been made to gas cooking equipment. The introduction of a gas supply to the hospital is a recent innovation. The Frenchay district on the outskirts of Bristol had hitherto been reliant for lighting and cooking on electricity or more primitive means and the strain on the electricity supply of the hospital has been for some time and still is, causing the committee no little anxiety. It was a prerequisite of any kitchen modernisation, therefore, that a supply of gas be negotiated with the Gas Board. This authority readily co-operated (although the nearest existing main was 900 yards from the hospital estate) and gas was first taken on 15th May, 1950. This facility was also welcomed in the expanding Area Pathological Laboratory at Frenchay and in the pharmacy departments which had previously to make do with a day-by-day supply of portable gas containers to feed their essential apparatus.
Oxygen Pipeline
Early in 1950 the consultant anaesthetists became increasingly exercised in mind concerning the inadequate and unsatisfactory arrangements at the hospital for the delivery, renewal and storage of medical gas cylinders. At present gas cylinders on delivery are deposited in a central store and porters collect empties three times daily from all sections, replacing with full cylinders. The high proportion of surgical cases in the hospital results in a rapid turnover of cylinders and moreover demands that a large reserve supply be held on each ward against the frequent and prolonged use of oxygen tents. Though the British Oxygen Company deliver five times weekly, the emergency call for supplies occurs more often than is desirable. It was recognised that the advantages accruing from a pipe-line system - instantaneous availability of oxygen at all times, economy in cost of the large capacity cylinders used in the manifolds and saving in porterage on transport and checking of daily deliveries - leave no doubt that a pipe-line system of supply is an essential feature of an up-to-date general hospital. Discussions were accordingly initiated with the medical staff, the committee's architect and representatives of the British Oxygen Company and Ministry of Works to consider the installation of a pipe-line system and in June, 1950, the management approved proposals for the provision of distribution points for oxygen and vacuum in Wards (varying in number between three and five per ward according to the nature of the accommodation), in X-ray departments and in the eight operating theatres and their corresponding anaesthetic rooms; nitrous oxide points to be provided only in theatres and anaesthetic rooms. An oxygen manifold of twenty four cylinders and nitrous oxide manifold of six cylinders is to be located in a central position. The capital cost is of the order of £4,500 and the project is now before the regional board.
Nurse Training
It may be considered a platitude to repeat that the backbone of hospital staffing is the student nurse and she (or he) must be of suitable temperament and personality. At the appointed day Frenchay Hospital had a place in the training of nurses merely to the extent of a limited affiliation by which three or four nurses at a time were seconded from another group for experience primarily on the venereal diseases wards; and a temporary recognition had been given for the purpose of an intensive training course for male nurses organised by the Ministry of Health. Of the nursing staff of the hospital, some 70 per cent. consisted of assistant nurses and ward orderlies. The Children's Orthopaedic Sanatorium was a recognised training school affiliated to a large general hospital outside the group. Other training facilities in the group were provided at Cossham Hospital (a general hospital of 101 beds) - again, in affiliation only. It was manifest to the management committee that their plans to develop at Frenchay a general hospital of 600 beds would come to naught if a complete nurse training scheme were not provided. The reputation of a hospital rests primarily on the competence of the nursing service which is rendered to its patients. In these days of fierce competition to obtain both trained staff and students, no hospital can hope to enter the front rank unless it can offer first-class training facilities and at least reasonable living accommodation to the type of student it is hoped to recruit. (This latter point will be referred to in more detail later.)
Accordingly the management gave early and serious thought to the question of how best to weld together the available teaching facilities of the group to present to the General Nursing Council an acceptable scheme of nurse training and, in October, 1948, remitted this matter to their nursing sub-committee for urgent attention. By May, 1949, a detailed scheme of recruitment and training on a modified block system had been drawn up and agreed with the principal matrons of the group and the regional nursing officer, the main requirements of the syllabus in general medicine and surgery, gynaecology and casualty being provided at Cossham Hospital; special surgery, paediatrics and geriatrics at Frenchay Hospital. The need for additional teaching staff was considered best met by the appointment of a tutorial head to take charge of the Group Training School and co-ordinate the group effort. Following approval by the management, the proposals were submitted to the General Nursing Council and the complete general training school received recognition on 22nd July, 1949. The committee were fortunate in obtaining as their tutorial head a senior member of the teaching staff of one of the leading London hospitals, who commenced duty on 1st October, 1949. The Preliminary Training School for the group is established at Frenchay and for practical teaching purposes award building surplus to bed requirements has been renovated and re-equipped thus giving the ideal layout.
Students, both men and girls, are admitted to the school in January, May and September, and during the last eighteen months recruitment has progressed in quantity and quality to the entire satisfaction of the management. There are now 130 students in training. As an adjunct of the main training scheme the management have also introduced pre-training facilities at Frenchay for girls who have reached 16years of age and intend to become student nurses. The problem of 'bridging the gap' is an old one and is well-known - there is no need to elaborate. Residential accommodation is as yet so limited that only living-out cadets can be recruited and the number is at present limited to six.
Residential Accommodation
Consideration of nurse-training leads one to the question of nurses, for students of the right type cannot be recruited or retained unless they can be resident. If accommodation be not available, then in the first place the net cannot be cast far and wide; secondly, such students as may be attracted are continually fighting a losing battle both as regards their daily travelling to and from the hospital and, more importantly, in the matter of study at home. We have suffered casualties on this account.
On taking over the two institutions the management found that accommodation was available for only 130 staff of all grades. However, the Ministry of Works had plans in hand for the adaptation of several blocks of buildings which would give a further ninety-seven rooms and these were handed over and occupation taken in February, 1950. With the gradual expansion of the hospital the race to keep the supply of residential accommodation ahead of the demand has been acute. This demand is twofold - on the one hand the nurse training scheme, now well into its stride, is attracting new students at the rate of 70-80 per year. The rapid programme of expansion is at the same time calling for increased numbers of trained nurses and domestics. Nor will the replacement of untrained ward staff by students alleviate the pressure on accommodation because the large number of ward orderlies who have hitherto comprised the majority of the ward staffs have always been non-resident.
Planning of New Nurses' Home
The problem was envisaged at the start, and in February, 1949, the committee's architect was commissioned to prepare plans for anew nurses' home to accommodate 350 persons. The proposal received the regional board's approval in principle in May, 1949. It is common with this kind of project that new ideas are propounded from time to time while planning is in progress and delays are inevitable. At Frenchay an unusual difficulty was experienced in that borings by the National Coal Board within half a mile of the hospital estate gave rise to fears -unduly exaggerated in some quarters - that the whole hospital was in danger of subsiding into the nether regions! It was, however, thought desirable by the committee's advisers to moderate the original scheme by reducing the building from eight storeys to three. A complete replanning was necessary and in the meantime the all-pervading financial stringency once again intruded. In the light of an intimation that not more than £250,000 of the capital moneys available could be allocated to a nurses' home at Frenchay, a further detailed assessment of immediate need was made. On this basis the architect has designed a building to give initially 100 rooms, but which will allow of extensions at a later date. At the time of writing this proposal is awaiting sanction to proceed with the preparation of working drawings.
Meantime, the management have to bridge the gap. All available accommodation was occupied when students of the May, 1951, preliminary training school came into residence. As the next step the committee have recently negotiated with the Bristol Corporation the purchase of a large country house in Frenchay village, the grounds of which are contiguous with the hospital and will conveniently become a part of the whole estate. Adaptations to these premises with some rearrangement of staff quarters will enable another twenty-five students to be accommodated. There only remain the schools of January and May, 1952, during which the training scheme will reach its peak. Plans to cope with this vital period are already under discussion.
Conclusion
The developments which have been described do not complete the management committee's picture of the hospital as they envisage its final form. Attention is now directed to a preliminary study of the expansion which will be demanded by X-ray services, medical records departments and pathological laboratories. These matters may come more clearly into view when the opportunity occurs at a later date to add another chapter to the story. Meantime one cannot conclude without placing on record the co-operation which has always been forthcoming from the ward sisters and other heads of sections during an extremely trying time. The period of waiting for better things tocome has been prolonged and somewhat exasperating, notwithstanding the excellent progress made. However, there is a feeling abroad at Frenchay Hospital that, to borrow a phrase from a more famous occasion, we have reached if not the beginning of the end, then the end of the beginning.The corners of the two blocks provide a common reference point in comparing the following photos.
January 1944 Winter 1950-51
September 1988 1990



As can be gathered from the above accounts, a great deal had been achieved in the six years or so from the end of the War. Nevertheless, a great more was needed. Vera Wilson's account of the next couple of years emphasises the evolutionary phases:
In September, 1950, the Regional Authorities were asked for a Speech Therapy Department to be established at Frenchay Hospital to benefit patients from the Neurosurgical Department suffering from speech, writing and reading disturbances, and for children in the Plastic Surgery Unit with speech defects due to congenital abnormalities. In October, 1951, a qualified full-time Speech Therapist was appointed.
Prior to the introduction of the National Health Service, planning for anew Frenchay Hospital had proceeded on the assumption that an exclusively specialised hospital would be developed. It was later decided that such a concept was impractical and the Management Committee formulated plans for broadening the scope of the hospital by allocating 100 beds for General Surgery and by providing a building, formerly used as a games room, to be converted into a twin operating theatre suite. These theatres were brought into use in September, 1951.
By 31st March, 1953, much had been achieved, and the beds allocated and in use were as follows:
Thoracic Surgery 120 (120)
Neurosurgery 80 (31)
Plastic Surgery 120 (94)
General Surgery (inc ENT) 100 (66)
General Medicine (inc TB) 160 (121)
Venereal Diseases 40 (42)
Staff Sick Bay 10 (9)
630 499
(Beds staffed and in use are in brackets)
The net average cost per patient per day was £2 12s 8d.
The new operating theatres and Neurosurgical extension were officially opened by Sir Geoffrey Jefferson, C.B.E., F.R.C.P.,F.R.C.S., F.R.S., on Wednesday,14th October, 1953. This new Unit consisted of four wards of 19 beds, an X-ray Department, offices for Neurosurgical staff, and a twin operating theatre suite with observation gallery.
Vera Wilson continues:

